{}
Background
- Definition: inhalation of gastric contents into the lung via passive regurgitation or active vomiting
- Common patients:
- “Full stomach”: Not NPO, bowel obstruction, pregnant, gastroparesis, intoxicated
- Incompetent LES: hiatal hernia, previous esophageal/gastric surgery, obese
- Can’t protect airway: ↓ LOC, residual NMB, neurologic disease
Considerations
- Signs/symptoms: Severe hypoxemia, ↑ peak insp. pressure, bronchospasm, ↑ tracheal/oropharyngeal secretions, chest retractions, dyspnea, coughing, laryngospasm, pulmonary edema
- ↑ morbidity/mortality: pneumonia, ARDS, sepsis, barotrauma
- CXR: infiltrates and atelectasis, but can be unremarkable
Risk Factors for Aspiration
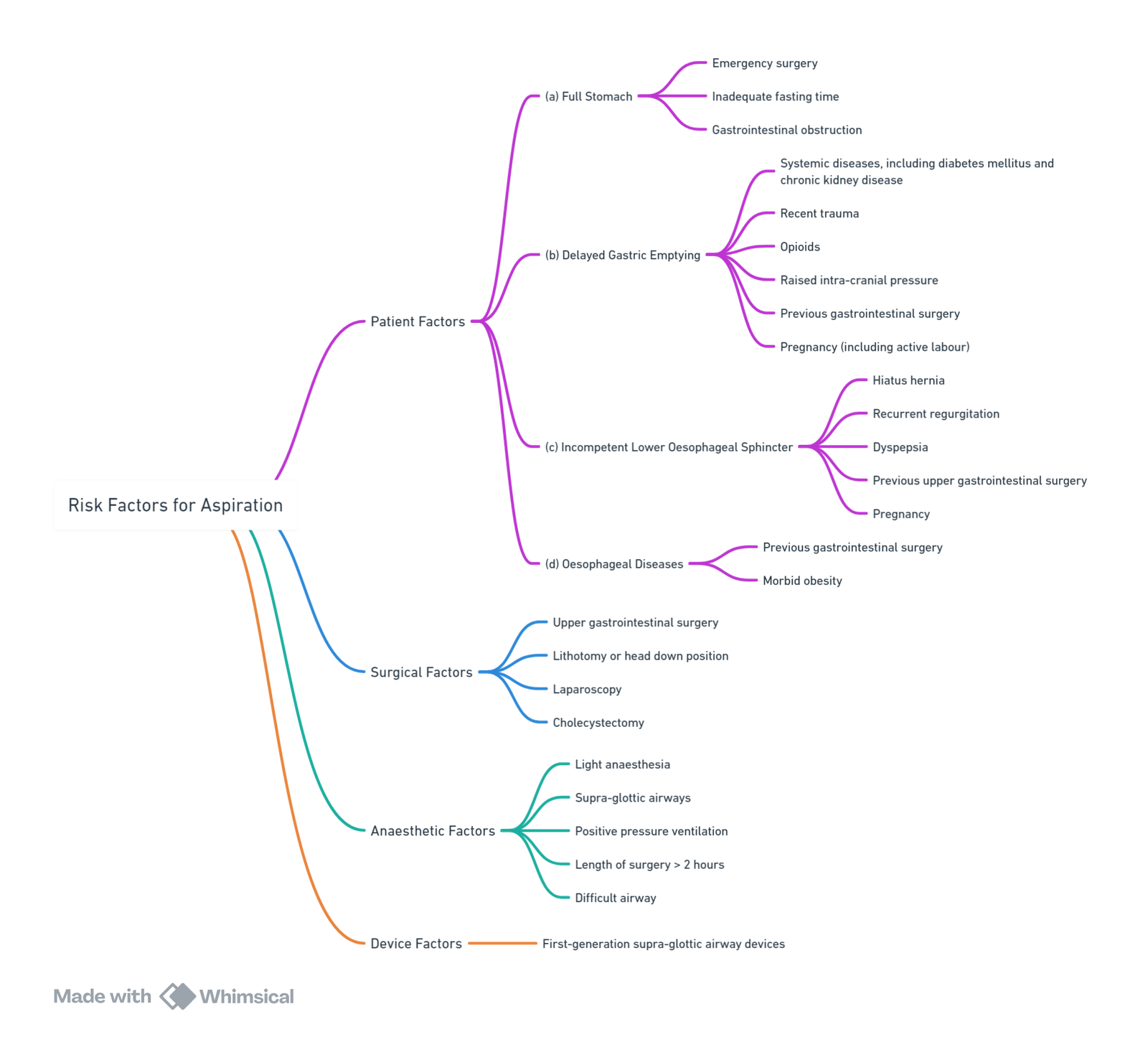
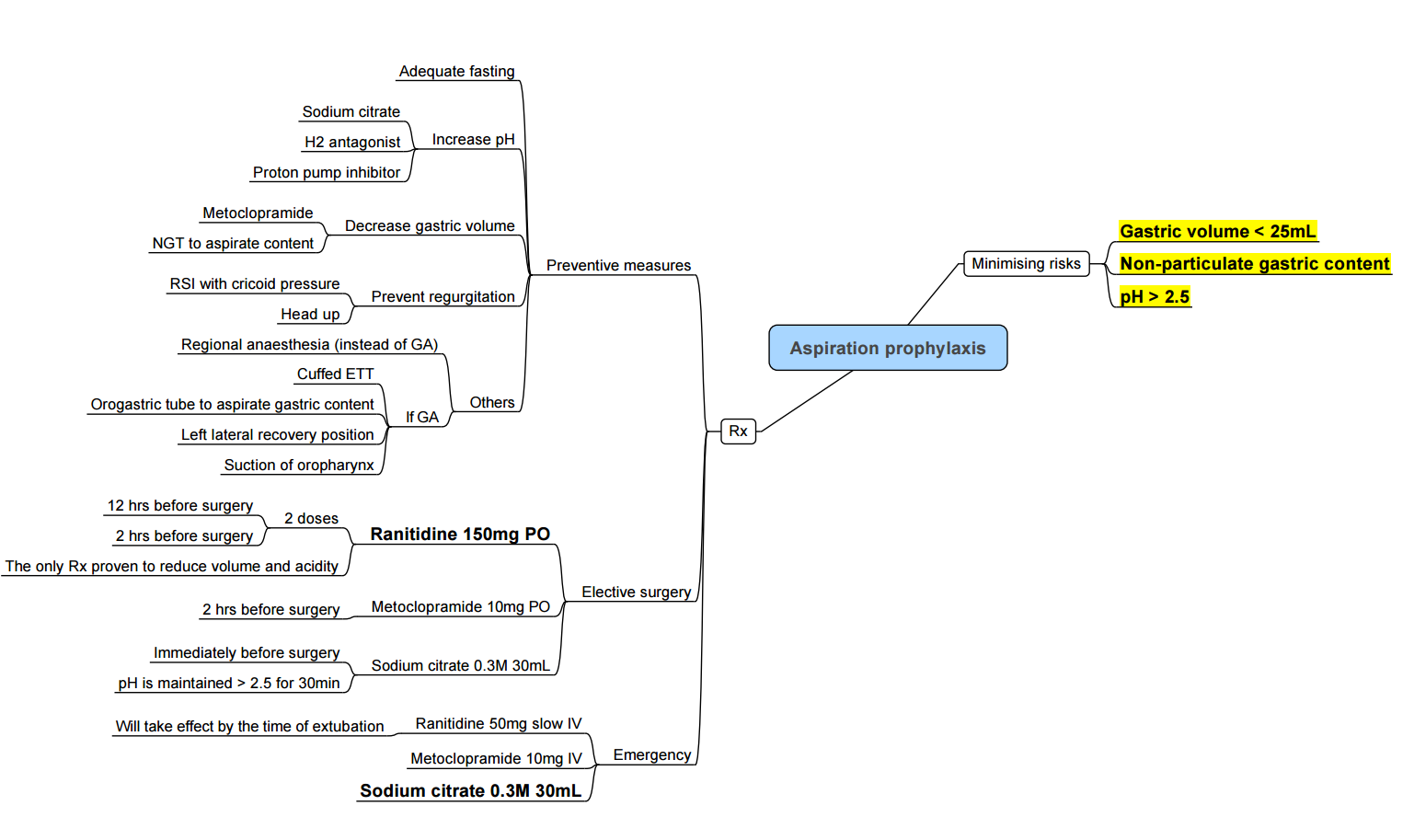
Strategies for Reducing Aspiration Risk
Extubation
- Awake after return of airway reflexes
- Position (lateral, head down, or upright)
Guidelines to Reduce the Risk of Aspiration
- Ensure experienced anaesthesia assistance is available at all times.
- Intubate all emergency cases.
- Apply appropriate cricoid pressure with all inductions using neuromuscular blocking agents.
- Intubate or seriously consider intubation in the following scenarios:
- Delayed gastric emptying (e.g., pregnancy, opioids, diabetes mellitus, renal failure)
- Increased intra-abdominal pressure (e.g., obesity, ascites, masses)
- Extubate high-risk cases awake and on their side. Extubate all others on their side.
Complications
- Obstruction (Particle-related)
- Pneumonitis (Inflammation – Acid-related)
- Infection (Bacterial)
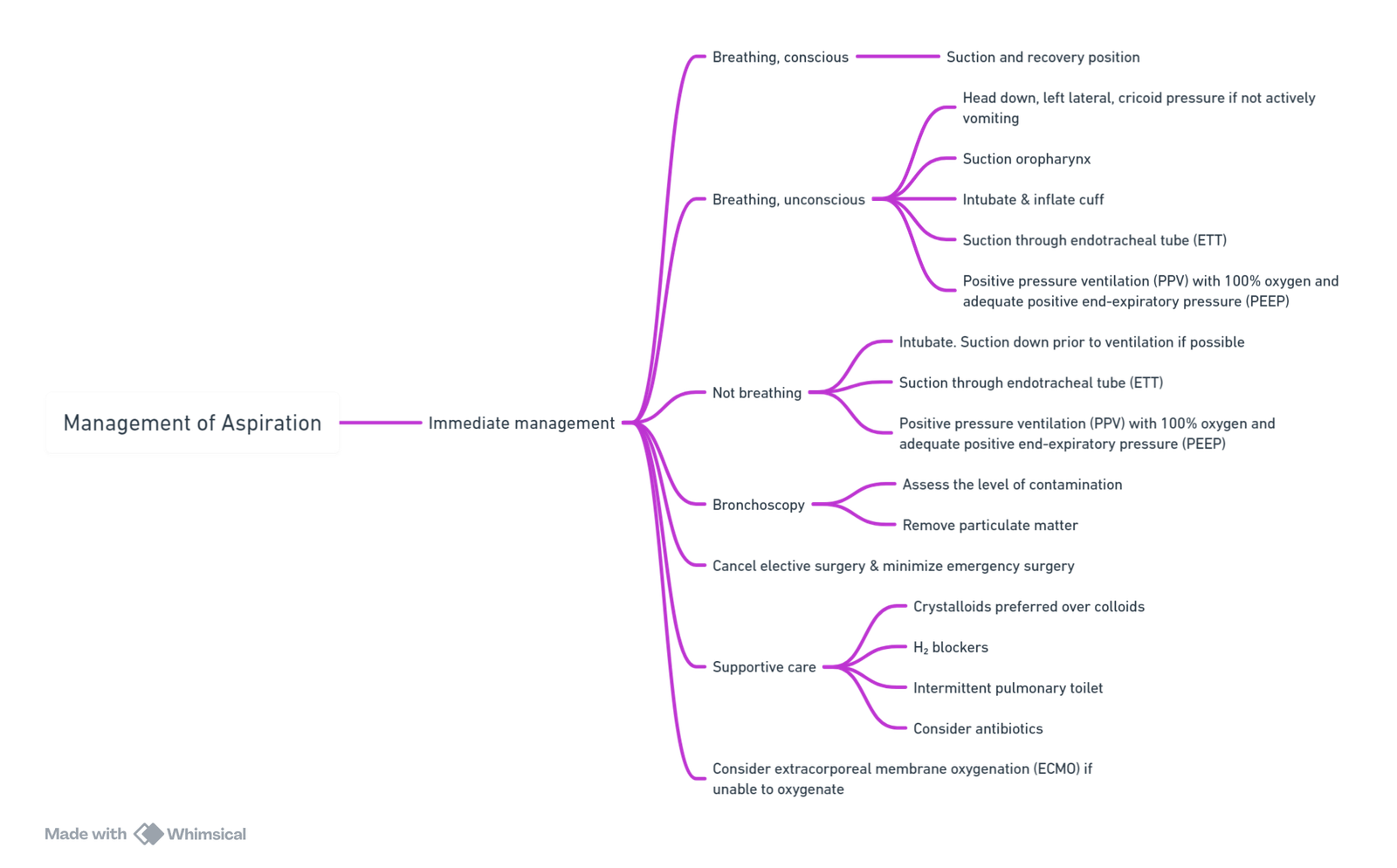
Management of Aspiration
Immediate Management
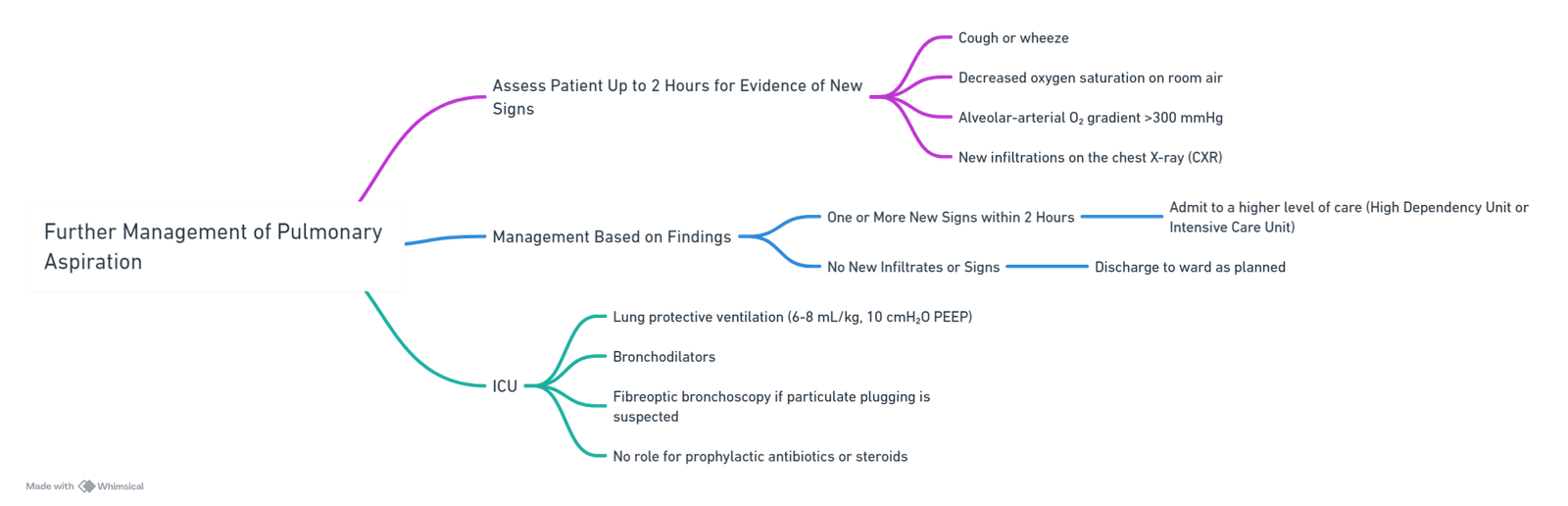
Further Management of Pulmonary Aspiration
Summary of Recommendations from NAP4 on Aspiration
- Patient Assessment
- All patients must be assessed for aspiration risk before surgery, especially urgent and emergency cases. In cases of doubt, assume the higher risk.
- Airway Management Strategies
- Strategies should align with the identified risk.
- Equipment and Skills
- Equipment and skills to detect and manage regurgitation and aspiration should be available at all times.
- Rapid Sequence Induction
- Remains the standard technique for airway protection.
- Cricoid Pressure Application
- Those applying cricoid pressure should be trained in its application and practice it regularly.
- Use of Supra-glottic Airways
- When tracheal intubation is not indicated, but a small increase in aspiration risk exists, consider using second-generation supra-glottic airways.
- Aspiration Reduction at Emergence
- Employ strategies to reduce aspiration risk if the patient is at risk.
- Blood Clot Aspiration Awareness
- Anaesthetists should be aware of the prevention, detection, and management of blood clot aspiration.
- Capnography and Blood Near Airway
- Take active measures when a flat capnography trace occurs after blood has been near the airway.
Links
References:
- Robinson, M. J. and Davidson, A. H. (2014). Aspiration under anaesthesia: risk assessment and decision-making. Continuing Education in Anaesthesia Critical Care &Amp; Pain, 14(4), 171-175. https://doi.org/10.1093/bjaceaccp/mkt053
- Anesthesia Considerations. (2024). Retrieved June 5, 2024, from https://www.anesthesiaconsiderations.com/
Summaries:
Copyright
© 2025 Francois Uys. All Rights Reserved.
id: “56c2e808-c5ad-45a0-8c00-38cf20e494c8”

