{}
Summary
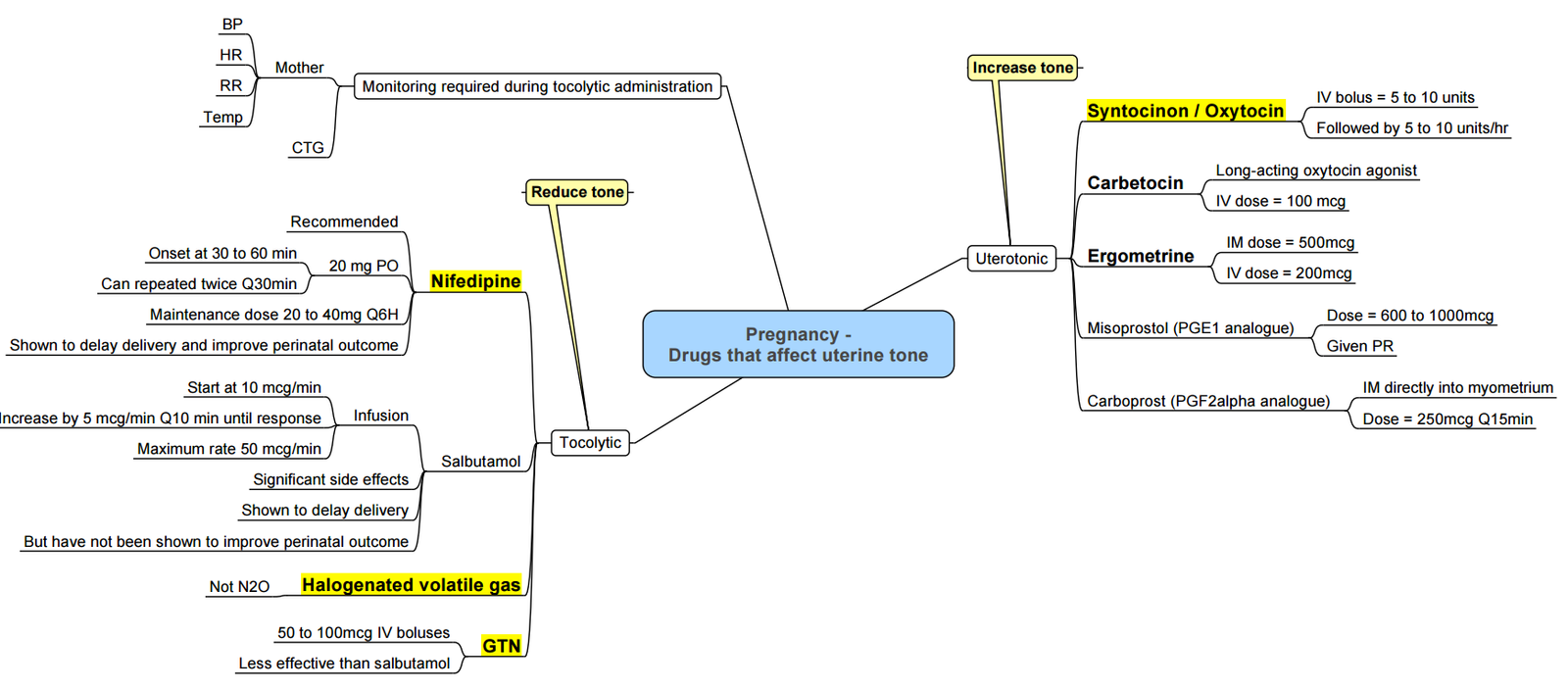
Oxytocic Agents
Overview
Oxytocic agents stimulate uterine contractions to prevent and treat postpartum haemorrhage (PPH) and manage the third stage of labour. Selection of agent and dose should balance efficacy and side effects, guided by patient risk factors and clinical setting.
Carbetocin
- Pharmacology: Synthetic oxytocin analogue; octapeptide with extended half-life (~40 min vs 4–6 min for oxytocin) due to resistance to enzymatic degradation.
- Efficacy: Single 100 µg IV bolus reduces PPH risk comparable to oxytocin infusion with fewer hypotensive episodes and need for additional uterotonics in elective caesarean delivery on meta-analysis.
- Dose: 100 µg IV over 1 min immediately after delivery. Heat-stable formulation recommended where cold chain unavailable.
- Side Effects: Similar to oxytocin (hypotension, headache, nausea); lower incidence of fluid overload and vasodilatation
Oxytocin
- Physiology: Endogenous nonapeptide hormone produced in hypothalamus, released from posterior pituitary; half-life 1–6 min.
- Mechanism: Binds uterine oxytocin receptors → ↑ intracellular Ca²⁺ → myometrial contraction.
- Indications: Active management of third stage of labour, induction/augmentation of labour, PPH prevention and treatment.
- Dosing (caesarean): 5 IU IV bolus over 2 min then 10 IU in 1 L crystalloid at 125 mL/h.
- Administration Tips: Give slow bolus to mitigate hypotension and reflex tachycardia; subsequent infusion if tone inadequate.
- Side Effects: Hypotension, tachycardia, water intoxication (antidiuretic effect), uterine hypertonicity, potential augmentation of succinylcholine neuromuscular block.
Ergometrine (Methylergometrine)
- Origin: Ergot alkaloid from Claviceps purpurea.
- Mechanism: Agonist at α‑adrenergic and 5‑HT₂ receptors → sustained uterine contraction and vasoconstriction.
- Dose: 200 µg IM; IV 100 µg slowly for severe atony (avoid rapid IV bolus).
- Contraindications: Hypertension, pre‑eclampsia/eclampsia, ischaemic heart disease, peripheral vascular disease.
- Side Effects: Severe hypertension, coronary vasospasm, nausea, vomiting, headache.
Misoprostol
- Pharmacology: Prostaglandin E₁ analogue; thermostable.
- Routes/Dose: 400–800 µg sublingual (preferred), 800 µg rectal, or 600 µg oral. Repeat once after 15 min if needed (max 800 µg).
- Use: Second-line or where injectable uterotonics unavailable.
- Side Effects: Fever, shivering, diarrhoea, abdominal pain.
Additional Prostaglandins
- Carboprost (15‑methyl PGF₂α): 250 µg IM every 15 min up to 2 mg (contraindicated in asthma).
- Sulprostone (PGE₂ analog): 500 µg IV infusion at 100 µg/h (max 1500 µg/24 h); side effects include hypotension, shivering.
International Consensus Recommendations
- Administer a prophylactic uterotonic (oxytocin or carbetocin) immediately after delivery of the anterior shoulder or fetus.
- Tailor initial dose—avoid “one-size-fits-all.”
- Use slow IV bolus of oxytocin (over ≥ 2 min) to reduce cardiovascular side effects.
- Consider carbetocin in high-risk or resource‐limited settings for single‐dose efficacy.
- Add second‑line agents early if tone remains inadequate.
- Individualise regimens for cardiac patients—dilute and titrate oxytocin, avoid ergometrine.
- Ensure clear labelling and distinct preparation of uterotonic syringes.
Use in Cardiac Disease
- Oxytocin: dilute (0.1 IU/mL), administer 0.1 IU increments; monitor blood pressure and uterine tone.
- Ergometrine: generally avoided; risk of severe hypertension and ischaemia.
- Misoprostol: acceptable with caution in IHD; minimal hemodynamic effects.
Links
- Ovarian hyperstimulation
- Anaesthetic management of specific cardiac conditions
- Maternal conditions
- Maternal collapse and CPR
- Obstetric haemorrhage
- Obstetrics Anticoagulation|Obstetrics Anticoagulation
References:
- Allman K, Wilson I, O’Donnell A. Oxford Handbook of Anaesthesia. Vol. 4. Great Clarendon Street, Oxford, OX2 6DP, United Kingdom: Oxford University Press; 2016.
- Butterworth J, Mackey D, Wasnick J. Morgan and Mikhail’s Clinical Anesthesiology, 7th Edition. 7th edition. New York: McGraw Hill Medical; 2022.
- B-Lynch C, et al. Uterotonic drugs for the prevention of postpartum haemorrhage. Cochrane Database Syst Rev. 2020;CD007358.
- Widmer M, et al. Heat-stable carbetocin versus oxytocin in preventing PPH: a randomised trial. Lancet. 2018;392(10155):1614–1620.
- RCOG Green-top Guideline No. 52: Prevention and Management of PPH. 2017.
- WHO. WHO Recommendations: Uterotonics for the Prevention of PPH. Geneva: WHO; 2018.
- Sangsawang B, Techatraisak K. Sublingual misoprostol for PPH prevention: meta-analysis. BJOG. 2019;126(11):1381–1389.
- Dyer RA, Butwick AJ, Carvalho B. Oxytocin for labour and caesarean delivery: implications for the anaesthesiologist. Curr Opin Anaesthesiol. 2011 Jun;24(3):255-61. doi: 10.1097/ACO.0b013e328345331c. PMID: 21415725.
- Heesen M, Carvalho B, Carvalho JCA, et al. International consensus statement on the use of uterotonic agents during caesarean section. Anaesthesia. 2019;74. In press
Summaries
—
Copyright
© 2025 Francois Uys. All Rights Reserved.
id: “76edf3e7-af7a-4ec6-956d-aae39066ea32”

