{}
Shoulder Surgery
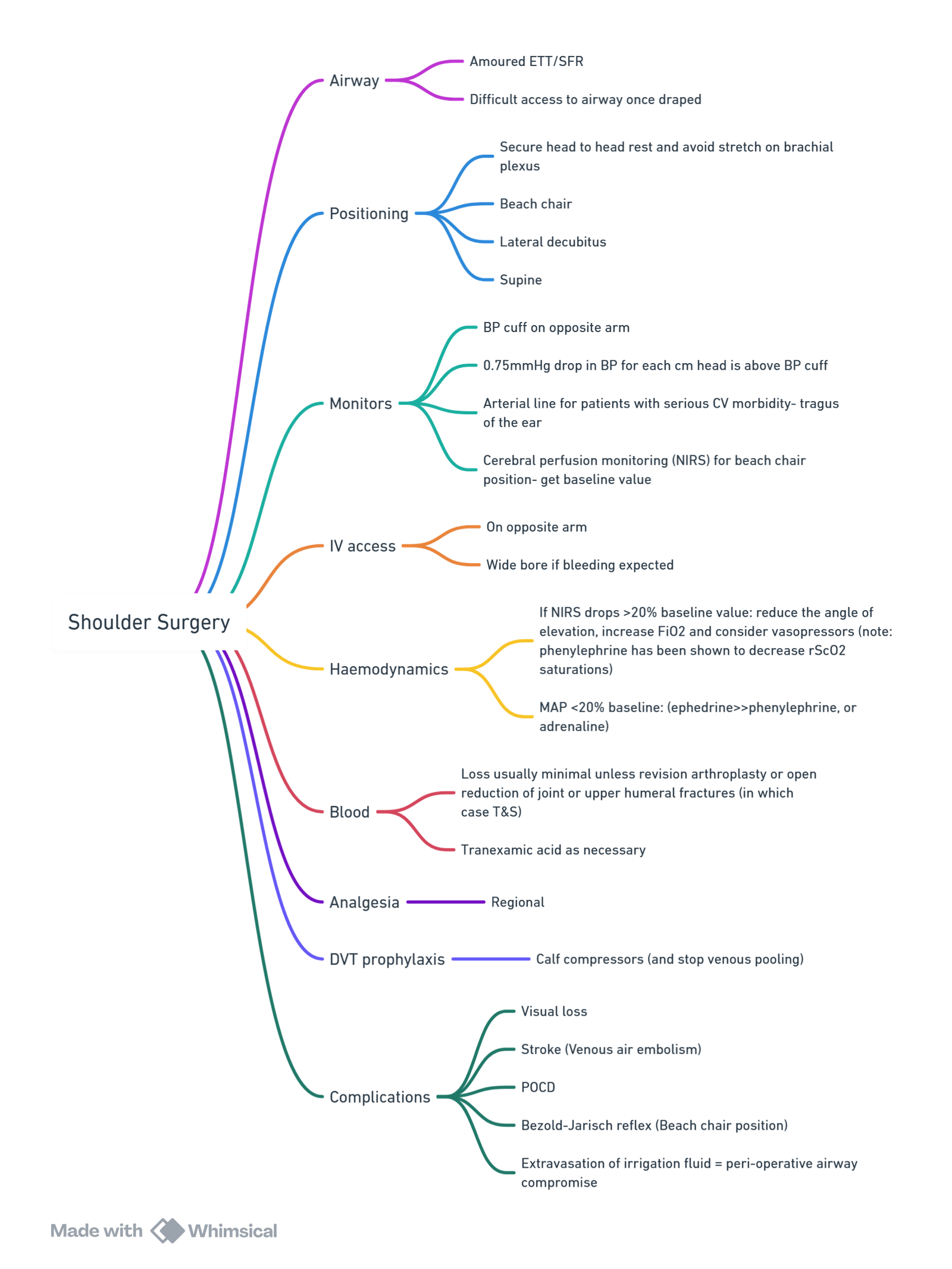
View or edit this diagram in Whimsical.
Introduction
- Arthroscopic or open shoulder procedures generate some of the highest early postoperative pain scores in orthopaedics; pain is greatest in the first 24–48 h but may persist for several days.
- Patient positioning (beach-chair or lateral decubitus) places the head away from the anaesthetist and necessitates meticulous airway security, long breathing circuits and extended IV tubing.
Pre-operative Assessment
| Issue | Relevance | Actions |
|---|---|---|
| Comorbidities | Rheumatoid arthritis (cervical instability), COPD/OSA, obesity, cardiac disease | Optimise cardio-respiratory status; discuss phrenic-sparing block if limited reserve |
| Antithrombotics | Regional anaesthesia & postoperative VTE prophylaxis planning | Follow latest ASRA 5th-edition antiplatelet/anticoagulant guidelines |
| Regional consent | Explain expected arm weakness, potential diaphragmatic paresis & rebound pain | Provide written information; outline rescue analgesia plan |
| Beach-chair risks | Cerebral desaturation, hypotensive-bradycardic events (HBEs) | Advise arterial line transduction at external auditory meatus for high-risk cases |
Conduct of Anaesthesia
Airway & Vascular Access
- Secure airway before positioning; south-facing armoured tube preferred for prolonged cases.
- Place wide-bore IV (contralateral arm) with 100 cm extension; consider second IV or arterial line for steep head-up tilt.
Anaesthetic Technique
| Component | Recommendation |
|---|---|
| GA | TIVA with propofol–remifentanil minimises cerebral autoregulatory impairment; remimazolam reduces hypotension on transition to beach-chair. |
| Regional | See below; combine with light GA or sedation for patient comfort and airway control. |
| Haemodynamics | Maintain brain-level MAP ≥ 70 mmHg (transducer at tragus); treat HBEs promptly with ephedrine/atropine. |
| Venous air embolism (VAE) | Rare but catastrophic; keep irrigation pumps < 50 mmHg, avoid air insufflation and monitor EtCO₂ for sudden drops.] |
Beach-chair Physiology
- CNS: 1 cm elevation of the head ≈ 0.75 mmHg fall in MAP; near-infrared spectroscopy (NIRS) detects cerebral desaturation events (CDEs) that occur in up to 56 % of cases under GA but seldom translate into stroke when MAP targets are respected.
- CVS: Venous pooling → ↓ preload, CO and CPP; mitigate with leg compression, slight hip-knee flexion, judicious fluids and vasopressors.
- Respiratory: FRC rises, but airway displacement risk increases—confirm tube position after final head-neck adjustment.
Regional Anaesthesia
| Technique | Analgesia Quality | Diaphragm Involvement | Key Evidence |
|---|---|---|---|
| Interscalene block (ISB) 15–20 mL 0.5 % ropivacaine | Gold-standard analgesia; lowest PACU opioid use | 70–100 % hemidiaphragmatic paresis | Urmey 1991; many RCTs |
| Superior trunk block (STB) 5–10 mL around C5-C6 trunk | Non-inferior pain scores & opioid consumption | 0–15 % paresis | 2023 meta-analysis of 4 RCTs (RR 0.07 for paresis) |
| Suprascapular + axillary (SSNB + ANB) 8–10 mL + 5 mL | Equivalent 24 h pain, higher intra-op opioid than ISB | < 5 % paresis | 2023 3-arm RCT (n = 118) |
| Continuous interscalene catheter | Longer analgesia (48 h); ↓ sleep disturbance | Same diaphragmatic effect as single-shot | 2019 review |
- Block selection guidance
- Normal pulmonary reserve: ultrasound-guided ISB (15 mL).
- Limited reserve (COPD, obesity, contralateral phrenic palsy): STB (8 mL 0.5 % ropivacaine) or combined SSNB + ANB.
- Anticoagulated patients: consider landmark-guided surgeon-delivered SSNB + ANB intra-articularly.
Post-operative Analgesia
| Time-frame | Recommended Regimen |
|---|---|
| PACU (0–6 h) | Paracetamol 1 g IV; dexamethasone 8 mg IV; ondansetron 4 mg IV; ketorolac 0.5 mg kg⁻¹ IV if not contra-indicated |
| 24 h | Continue paracetamol 1 g 6-hourly; NSAID 8-hourly; rescue oral oxycodone 0.05 mg kg⁻¹; consider gabapentin 300 mg nocte for high opioid tolerance |
| Catheter techniques | Continuous ISB: ropivacaine 0.2 % 5 mL h⁻¹ with 5 mL bolus q30 min; Subacromial catheter: 10 mL 0.25 % bupivacaine q4 h equally effective in rotator cuff repair |
Early mobilisation with the elbow supported reduces swelling and improves analgesia. Educate patients about block resolution and rebound pain; supply rescue analgesics before discharge.
Complications & Prevention
| Complication | Prevention |
|---|---|
| Cerebral desaturation / stroke | Maintain brain-level MAP ≥ 70 mmHg; NIRS monitoring; avoid excessive head flexion |
| Hypotensive-bradycardic events | Adequate preload; avoid large propofol/dexmedetomidine boluses; atropine/ephedrine ready |
| Hemidiaphragmatic paresis | Use STB or SSNB + ANB in high-risk lungs |
| VAE | Limit arthroscopic pump pressures; avoid air; monitor EtCO₂ |
| Nerve & pressure injuries | Pad head, arms, ischial tuberosities; minimise neck rotation; arms in padded gutters |
Links
References:
- Hewson, D. W., Oldman, M., & Bedforth, N. (2019). Regional anaesthesia for shoulder surgery. BJA Education, 19(4), 98-104. https://doi.org/10.1016/j.bjae.2018.12.004
- Beecroft, C. and Coventry, D. (2008). Anaesthesia for shoulder surgery. Continuing Education in Anaesthesia Critical Care &Amp; Pain, 8(6), 193-198. https://doi.org/10.1093/bjaceaccp/mkn040
- Amaral S, Lombardi RA, Medeiros H, et al. Superior trunk block as a phrenic-sparing alternative to interscalene block: systematic review and meta-analysis. Cureus. 2023;15:e48217. pubmed.ncbi.nlm.nih.gov
- Kim DH, Lin Y, Beathe JC, et al. Superior trunk block versus interscalene block for shoulder surgery: randomised trial. Anesthesiology. 2019;131:521-533. pubmed.ncbi.nlm.nih.gov
- Boekel P, Brereton SG, Doma K, et al. Surgeon-directed suprascapular + axillary nerve blocks versus interscalene block: 3-arm RCT. JSES Int. 2023;7:307-315. pubmed.ncbi.nlm.nih.gov
- O’Neill CN, McFarland K, Bowyer A, et al. No increased risk of cerebrovascular accident with beach-chair versus lateral positioning for shoulder arthroscopy. Arthrosc Sports Med Rehabil. 2023;5:100826. pmc.ncbi.nlm.nih.gov
- Gould HP, Yadeau JT, Fields KG, et al. Risk of intra-operative cerebral oxygen desaturation in beach-chair shoulder surgery. Clin Orthop Relat Res. 2021;479:2680-2694. pubmed.ncbi.nlm.nih.gov
- Hong JY, Choi SJ, Park K, et al. Risk factors for hypotensive-bradycardic events during shoulder arthroscopy in sitting position. Korean J Anesthesiol. 2020;73:201-208. ekja.org
- ee MG, Shin YJ, You HS, et al. Effects of low-volume superior trunk block on diaphragmatic function. Anesth Analg. 2021;133:1303-1310. pubmed.ncbi.nlm.nih.gov
- Urmey WF, Talts KH, Sharrock NE. Hemidiaphragmatic paresis after interscalene block diagnosed by ultrasound. Anesth Analg. 1991;72:498-503. (Historical reference for 100 % paresis with ISB).
Summaries:
Copyright
© 2025 Francois Uys. All Rights Reserved.
id: “89c1fb6e-1d25-4cf9-8fcf-ddd4cae6374a”

