{}
Long Volume Reduction Surgery
Rationale for Lung Volume Reduction Surgery (LVRS)
Possible reasons for clinical improvements in patients who undergo LVRS include:
- Resection of Poorly Functioning, Overdistended Lung Tissue:
- Provides room for expansion of better-functioning lung that has been compressed.
- Recruitment of lung with better elastic recoil and less expiratory flow limitation leads to improved FEV1 and reduced ventilation-perfusion mismatch.
- Reduction in Lung Volume:
- Corrects the effects of hyperinflation on the chest wall and diaphragm.
- Enhances the efficiency of respiratory muscles and reduces the work of breathing.
- Impact on Cardiac Function:
- Dynamic hyperinflation of the lung exerts an effect similar to cardiac tamponade.
- LVRS may enhance cardiac function and performance by decreasing intrathoracic pressure.
- Systemic Effects:
- Improved systemic endothelial function and reduced systemic arterial pressure have been demonstrated after LVRS.
Perioperative Approach
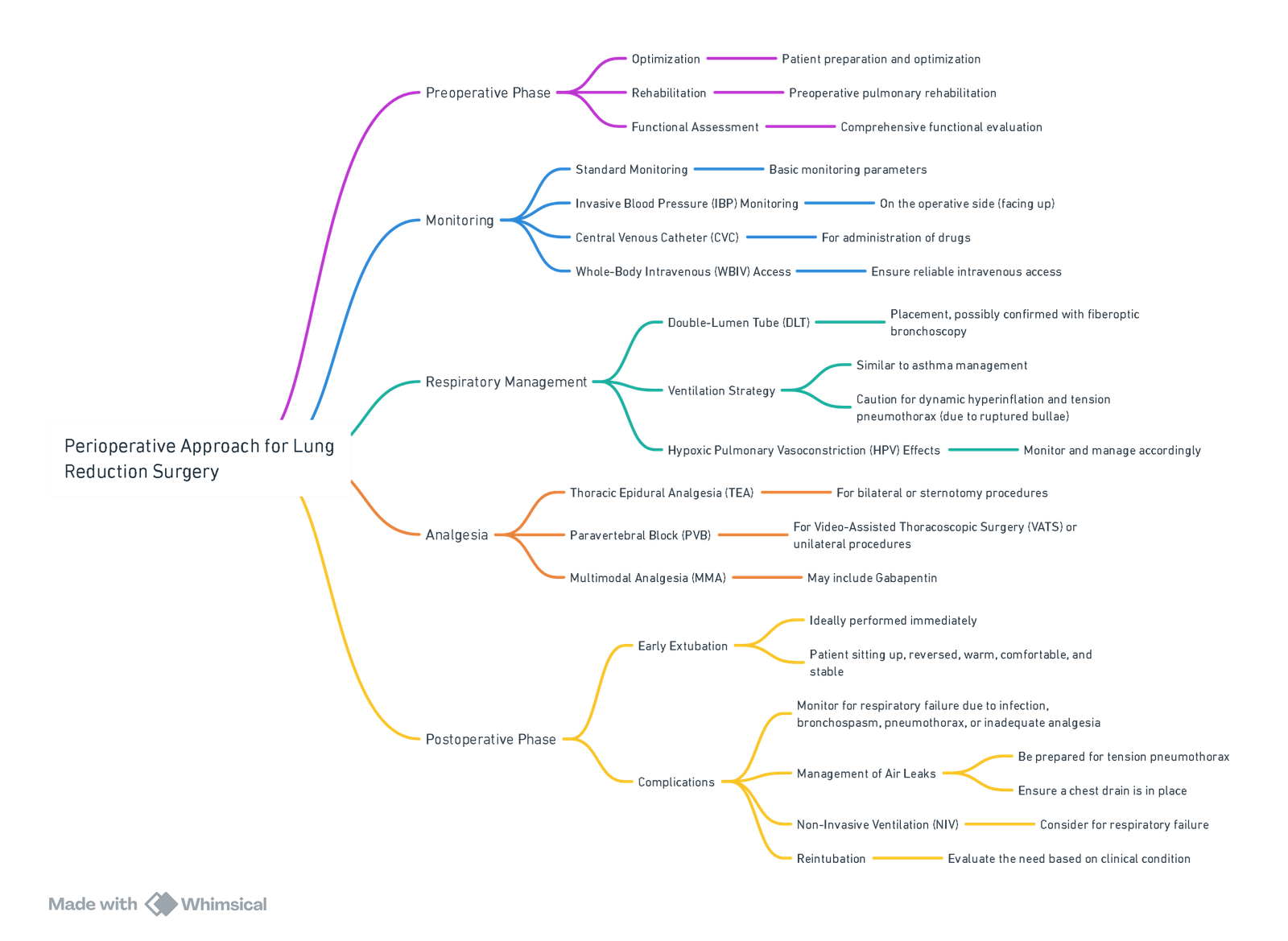
View or edit this diagram in Whimsical.
Rationale for Specific Preoperative Tests in Patients Considered for Lung Volume Reduction Surgery (LVRS)
| Preoperative Test | Rationale |
|---|---|
| Echocardiography and Coronary Angiography | To assess cardiac function and identify significant pulmonary hypertension, which might contraindicate surgery. Significant coronary artery disease, heart failure and ejection fraction <40% are comorbidities that increase surgical mortality. |
| Lung Function Tests | Forced expiratory volume in 1 s (FEV1) expected to be <45% of predicted. DLCO expected to be between 20% and 40% of predicted. Patients will often have a residual volume >150% of predicted. Total lung capacity is often >100% predicted. A marked abnormality of alveolar gas exchange (DLCO<20%) or a FEV1 <20% of predicted are contraindications for LVRS. |
| High Resolution CT of Chest | To identify if the lungs are suitable for surgery (i.e. a heterogeneous distribution of emphysema in which there are areas of relatively normal lung tissue). Homogeneous distribution of emphysema without areas of preserved lung, presence of large bullae, interstitial lung disease and nodules are contraindications to LVRS. |
| Cardiopulmonary Exercise Testing | To determine cardiopulmonary functional status and to assess potential operative risk. To quantify and monitor clinical response to surgery. A pharmacological stress test is advisable if an exercise test cannot be performed. |
| Shuttle Walk Test | A distance of 150 m is an accepted minimum requirement post pulmonary rehabilitation. |
Links
- One lung Ventilation and VATS
- Double lumen and Bronchial blocker
- Hypoxia Pulmonary Vasoconstriction (HPV)
- Respiratory physiology and Thoracic anaesthesia
- Thoracic pre-op assessment
- Lung resection
- Whole lung lavage
References:
- Anaesthesia for lung volume reduction surgery and endobronchial valves – BJA Education. https://www.bjaed.org/article/S2058-5349(18)30049-0/fulltext
- Elayaperumal, A. and Jackson, R. (2018). Anaesthesia for lung volume reduction surgery and endobronchial valves. BJA Education, 18(7), 193-198. https://doi.org/10.1016/j.bjae.2018.04.002
- James, M. F. M. and Dyer, R. A. (2005). Anaesthesia for lung volume reduction surgery. Southern African Journal of Anaesthesia and Analgesia, 11(3), 103-106. https://doi.org/10.1080/22201173.2005.10872408
Summaries:
Copyright
© 2025 Francois Uys. All Rights Reserved.
id: “2d467d5a-55dc-46f9-8a35-08a5b4da1be1”

